
Calcific Tendonitis in the Shoulder
Last Updated on August 12, 2024 by The SportsMD Editors
Calcific tendonitis in the shoulder is characterized by the presence of calcium deposits, actually hydroxyapatite (crystalline calcium phosphate), in a tendon of the rotator cuff. It’s often asymptomatic and occurs in 3-20% of shoulders in the general population.
When symptomatic it has a variable presentation of shoulder pain. It may be aggravated by elevation of the arm above shoulder level or lying on the shoulder. Patients may also complain of stiffness, snapping, catching, or weakness. It is most commonly found in adults between the ages of 30-50 years. Women, especially housewives and clerical workers, are more commonly affected than men.
Calcific Tendonitis Causes?
Calcific tendonitis causes are is not well understood. It is not believed to be caused by trauma or systemic disease and is rarely associated with rotator cuff tears. Some researchers think calcium deposits form because there is not enough oxygen to the tendon tissues. Others feel pressure on the tendons can damage them, causing the calcium deposits to form. Reactive calcification occurs in younger patients and seems to go away by itself in many cases.
Calcific Tendonitis stages
- Calcific tendonitis formative stage: fibrocartilagenous transformation of a portion of the rotator cuff tendon with subsequent calcification – with a dry and chalky appearance.
- Resting stage: mature-appearing deposits, minimal pain, possible mechanical symptoms
- Resorptive stage: calcium deposit is resorbed by inflammatory reaction – deposits have the appearance of toothpaste and may leak into the subacromial bursa and may be extremely painful
- Postcalcific stage: fibroblasts reconstitute the tendon after the calcium deposit has been resorbed and pain subsides
Diagnosis of Calcific Tendonitis
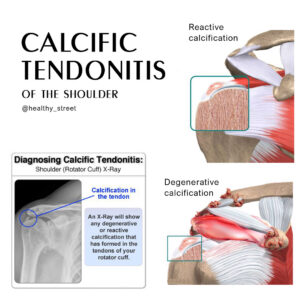
 Plain x-rays may demonstrate asymptomatic calcium deposits in the rotator cuff tendons. Symptoms often occur if the calcification deposit is larger than 1.5cm. Calcium deposits may also be seen on ultrasound and MRI.
Plain x-rays may demonstrate asymptomatic calcium deposits in the rotator cuff tendons. Symptoms often occur if the calcification deposit is larger than 1.5cm. Calcium deposits may also be seen on ultrasound and MRI.
Calcific Tendonitis Shoulder Treatment
Most patients seek calcific tendonitis treatment during the painful resorptive phase. Treatment during other phases, during which the calcium deposits are generally asymptomatic, should be directed at other possible pathological conditions of the shoulder. There are several treatment options used for calcific tendinitis.
Non-operative management is the treatment of choice. Physical therapy is often prescribed to maintain or regain shoulder range of motion and strength.
Corticosteroids may be injected into the subacromial space to reduce inflammation and control pain. Shoulder Calcific Tendonitis Treatment varies based on the clinical and radiographic stage of the calcification. In the resorptive phase needling, aspiration, and lavage may be successful in achieving pain relief. The calcium deposits are localized by ultrasound or fluoroscopy and are broken up by repeated puncturing with a needle and then the deposits, appearing toothpaste-like, are removed by injecting and aspirating saline with a syringe. In the formative or resting phases another treatment option used to break up the deposits is extracorporeal shock wave therapy (ECSW).
Home Remedies
There are several home remedies that can help alleviate Calcific Tendonitis Shoulder pain, such as P.R.I.C.E Treatment:
- Protection: The purpose of protection is to avoid further injury to the area by protecting the injured structures. The type of protection used varies depending on the injured area but may include an ace bandage, aluminum splint, sling, protective tape, or over-the-counter brace.
- Rest: The purpose of resting is to allow the body’s own healing processes to naturally occur without being impeded by movement of the injured area. Any increase in movement of an injured tissue results in increased circulation to the area which in turn may result in further damage to the injured tissue and/or increased swelling.
- Ice: Ideally, ice packs are made of crushed ice because the crushed ice is more comfortable for the athletes and conforms to the contours of the injured area better than cubed ice. Ice can be placed into plastic or Ziploc bags. A light barrier should be placed between the skin and the ice bag (paper towel) to prevent injury to the skin during the application of the ice.
The ice pack can be secured with an ace bandage if needed. The ice should be applied for 20 minutes at a time and then removed. This can be repeated every two hours while the athlete is awake.
- Compression: When the ice pack is removed, a compression wrap should be applied to the injured area. The compression wrap serves as a mechanical barrier so that swelling is minimized in the injured area. There are a number of compression wraps available on the market, but the most commonly used is an elastic or ace bandage.
- Elevation: Elevation is important immediately post-injury to reduce the amount of blood flow to the injured area.
Following the PRICE principles is an effective way to minimize the swelling in an injured area so that the athlete can return to play quickly.
Get a Virtual Sports Specialized appointment within 5 minutes for $29
 When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments are within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments are within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
Calcific Tendonitis Surgery
 Calcific tendonitis surgery of the shoulder with arthroscopy may be indicated if symptoms progress, pain is constant and interfering with activities of daily living, or there is a failure to improve with conservative management. The calcium deposits are localized and removed from the rotator cuff tendons with an arthroscopic shaver or through a longitudinal incision in the tendon. The rotator cuff may require repair after a thorough debridement. An acromioplasty is often performed during the arthroscopy to increase the amount of space between the acromion and rotator cuff tendons. This allows for easier shoulder movement which prevents impingment and subsequent pain and inflammation.
Calcific tendonitis surgery of the shoulder with arthroscopy may be indicated if symptoms progress, pain is constant and interfering with activities of daily living, or there is a failure to improve with conservative management. The calcium deposits are localized and removed from the rotator cuff tendons with an arthroscopic shaver or through a longitudinal incision in the tendon. The rotator cuff may require repair after a thorough debridement. An acromioplasty is often performed during the arthroscopy to increase the amount of space between the acromion and rotator cuff tendons. This allows for easier shoulder movement which prevents impingment and subsequent pain and inflammation.
Prognosis after Calcific Tendonitis
Early, aggressive physical therapy is started on the first postoperative day to regain shoulder range of motion and prevent stiffness. If an extensive debridement is performed with rotator cuff repair the postoperative rehabilitation program will be similar to that after a rotator cuff repair. Pain relief after debridement of the calcium deposits is usually substantial. After arthroscopic debridement of calcium tendinitis 70% of patients are noted to be pain-free at 3 months postoperatively and 90% are pain-free at 4 years postoperatively. Calcification has been reported to recur in 16-18% of patients.
References:
- Azar, Frederick M. Shoulder and Elbow Injuries: Calcific Tendinitis, Campbell’s Operative Orthopaedics, 10th Edition, 2003. 2352-2355.
- Woodward, Anthony H. Calcifying Tendinitis. EMedicine 2006.





