
Chronic traumatic encephalopathy
Last Updated on August 12, 2024 by The SportsMD Editors
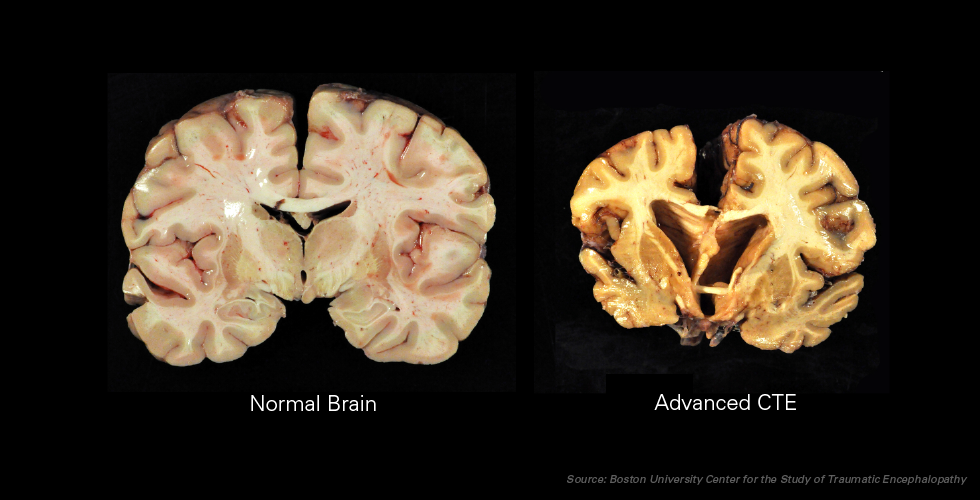
Chronic traumatic encephalopathy (CTE) is a degenerative brain disease that results in behaviors similar to Alzheimer’s disease (AD). However, according to researchers, CTE has a clear environmental cause (repeated brain trauma) rather than a genetic cause. In other words, CTE is the only preventable form of dementia.
Originally termed “dementia pugilistica” otherwise known as “punch drunk”, this disorder was first described in 1928 in boxers because boxers suffered from slowed movement, confusion, speech problems, and tremors (Sports Legacy Institute, 2010).
Although only recently termed chronic traumatic encephalopathy (first documented in the medical literature in 1996), CTE is now the preferred medical term for this disease.
The disease is characterized by a number of neurological and physiological changes in the brain including the buildup of an abnormal protein called tau. This protein builds up in places in the brain where it is not supposed to be and congregates in clumps in and around the brain disrupting its function.
Classifications of chronic traumatic encephalopathy
The clinical symptoms associated with CTE vary in severity depending on which clinical stage the individual is in (McKee, A.C., et. al., 2009). Initial symptoms include the following:
• Deterioration in attention, concentration, memory
• Disorientation
• Confusion
• Dizziness
• Headaches
• Lack of insight
• Poor judgment
• Overt dementia
• Slowed muscular movements
• Staggered gait
• Impeded speech
• Tremors
• Vertigo
• Deafness
The individual may progress through three stages of the disease beginning in the first stage with affective disturbances and psychotic symptoms. As the disease progresses to stage two, the individual may suffer from social instability, erratic behavior, memory loss, and the initial symptoms of Parkinson’s disease (McKee, A.C., et.al., 2009).
The final stage consists of a progressive deterioration to dementia and may have other symptoms including the signs associated with Parkinson’s disease, speech difficulties, gait abnormalities, dysarthria (speech disorder characterized by neuromuscular weakness or lack of control of facial muscles), dysphagia (difficulty swallowing), and ptosis (drooping eyelid) (McKee, A.C., et.al., 2009).
Diagnosis for chronic traumatic encephalopathy
Unfortunately, at this time, there are no specific markers or tests to detect CTE in a living athlete. Currently, CTE is diagnosed by studying brain tissue under a microscope after death.
Update November 16, 2017 –
Doctors were successfully able to diagnose a living person with chronic traumatic encephalopathy (CTE), a first for the field of medical research, according to a recently published article.
The findings, released in the medical journal Neurosurgery on Nov. 10, said an autopsy on the brain of a retired NFL player confirmed the results of scans taken more than four years before the subject died. CTE is “a progressive degenerative disease of the brain found in people with a history of repetitive brain trauma,” according to the Research CTE Center at Boston University.
https://twitter.com/MtnHousePsych/status/932454613407604736
Who gets chronic traumatic encephalopathy?
Although initially seen primarily in professional boxers, cases have now been identified in a number of athletes competing in different sports. According to Mckee et al. (2009), of the 51 confirmed cases of CTE, 90% of the cases occurred in athletes. The athletes included the following:
• 39 amateur and professional boxers
• 5 football players
• 1 professional wrestler
• 1 soccer player
Furthermore, statistics from the Center for the Study of Traumatic Encephalopathy (CSTE) identified that 17 of the 18 deceased contact sport athletes studied showed evidence of CTE (Sports Legacy Institute, 2010).
Because repetitive closed head injuries seems to be the cause of CTE, athletes involved in contact sports may be at risk including athletes in the sports of football, boxing, wrestling, rugby, hockey, lacrosse, soccer, and skiing. CTE has also been identified in “epileptics, headbangers, and domestic abuse victims” (Mckee, A.C., et. al, 2009).
While athletes in collision sports (football and boxing) may sustain higher numbers of concussive and subconcussive brain injuries, any athlete in any sport who may have sustained more than one concussive injury may be at risk for CTE.
CTE, was found in 99% of deceased NFL players’ brains that were donated to scientific research, according to a study published July 25, 2017 in the medical journal JAMA. The JAMA study is the largest of its kind and all of those studied were required to have football as their primary exposure to head trauma. The criteria for submitting a brain was based on exposure to repetitive head trauma, regardless of whether that individual exhibited symptoms during their lifetime.
Out of 202 deceased former football players total — a combination of high school, college, and professional players — CTE was neuropathologically diagnosed in 177, the study said. The disease was identified in 110 out of 111 former NFL players. It was also found in three of the 14 high school players and 48 of the 53 college players.
Unfortunately, at this time, there are no specific markers or tests to detect CTE in a living athlete. Currently, CTE is diagnosed through studying brain tissue under a microscope. This means that there is no way to tell if an athlete with a history of concussions is at risk for CTE.
Causes of chronic traumatic encephalopathy
Unfortunately, the research is not at the point to determine the exact number of concussive injuries it takes to initiate permanent brain deterioration. What is known is that repetitive brain injury causes CTE. The questions that need to be answered include:
• How many concussions does it take to cause CTE?
• What severity of concussions causes CTE?
• How many years of repetitive concussions does it take to cause CTE?
• How many years after an athlete receives his/her last concussion does CTE begin to deteriorate the brain?
• Is CTE manifested uniquely in each individual athlete?
• Do different athletes have different tolerances for developing CTE?
A lot of questions need to be answered. Fortunately, the Center for the Study of Traumatic Encephalopathy was created in 2008 for the sole purpose of conducting research to determine the neuropathology and pathogenesis of CTE. Once the pathology of the disease is better understood, then the risk factors can be identified along with how to prevent and treat this disease.
According to a press release by one of the co-directors of CSTE, Dr. Robert Stern, a large study is underway involving a number of former NFL players to study their lives and then examine their brains following their death. To this end, more than 250 current and former athletes, including 60 retired NFL players, have agreed to donate their brain and spinal cord to the CSTE upon death (CSTE Press Release, 2010).
In a study of 111 brains of NFL players, 110 had CTE, the degenerative disease caused by repeated blows to the head https://t.co/WL2utpi7FY pic.twitter.com/12QjlqxtaN
— The New York Times (@nytimes) July 26, 2017
The study found CTE in 99 percent of brains obtained from National Football League (NFL) players, as well at 91 percent of college football players and 21 percent of high school…https://t.co/mKs6cLbBjn
— M (@Matosan15) January 8, 2023
Prevention chronic traumatic encephalopathy
Because the cause of CTE is known, the prevention of CTE needs to focus on the proper diagnosis and management of athletes who have sustained concussions along with adhering to guidelines before returning to play. Unfortunately even with the advances lately in the management of concussion, they may not be enough.
According to a recent statement by Dr. Robert Stern, co-director of CSTE, new evidence shows” that 85% of concussions require about three weeks of recovery” (Abel, D., 2010). This is a longer time period than anything currently in the literature for return to play guidelines.
Current guidelines recommend a graduated increase in the level of activity of the athlete progressing from the initial stage of “light exercise” towards “full contact” activity once the athlete is completely symptom-free at rest. The athlete progresses through each stage as long as the athlete remains symptom-free during each stage. If symptoms return, then the athlete needs to stop for the day. This progression may be completed in as little as 5 days or may take as long as the athlete requires.
More research needs to be conducted to ensure that the current neurological tests that are being used in the field are accurate and correspond correctly to the state of the brain. If concussed athletes’ brains still suffer the effects of being concussed without corresponding outward signs or symptoms, then better neurocognitive tests need to be created to accurately reflect the status of the brain.
While the researchers continue to study the effects of concussions on athletes’ brains, lawmakers have moved to take the issue into their own hands by creating laws that would better protect young athletes. Bills have been introduced across this country in a number of states (i.e., California, New York, Massachusetts) to protect athletes who have been concussed by not allowing these athletes to return to play on the same day of the injury, requiring medical approval before concussed athletes are allowed to return to their sport, and by introducing training and education for coaches, athletic administrators, parents, and athletes as to the dangers of concussions (Abel, D., 2010).
Dr. Robert Stern offers his own recommendations specifically for the sport of football including reducing full-contact practices, changing the way players line up on the field, and using new helmets to reduce the force of the impact on the football players’ brains (Abel, D., 2010).
The best recommendations for the prevention of CTE is to ensure that athletes who sustain concussions be seen by sports medicine professionals who have experience in treating concussions. Because the research on concussions has changed significantly over the past several years, primary care physicians who do not specialize in sports medicine might not be aware of how to correctly diagnose a concussion using the latest guidelines, utilize the new diagnostic tools, and how to apply current treatment protocols.
Parents need to also be educated as to the signs and symptoms of concussion and be diligent to learning the current treatment protocols also. Parents may be in the best situation to detect subtle changes in their child’s behavior that others may not notice.
Last, it is the parents’ and the coaches’ responsibility to ensure that no athletes return to sport until they are completely symptom free of all signs and symptoms of concussion at rest and with full activity. Returning an athlete too early to sport after a concussion may also place the athlete at risk for second impact syndrome (life threatening brain injury).
Treatment for chronic encephalopathy
Because this disease has not been able to be detected until after the death of the athlete, it is not an area that has received attention until recently. As researchers better understand the progression of CTE and its effect on the brain, researchers can then begin to focus on treatment protocols.
Find a Doctor who specializes in Chronic Traumatic Encephalopathy:
National Institute of Neurological Disorders and Stroke
P.O. Box 5801
Bethesda, MD 20824
Toll-Free: 1-800-352-9424
http://www.ninds.nih.gov/
American Academy of Neurology (AAN)
1080 Montreal Ave.
St. Paul, MN 55116
Toll-Free: 1-800-879-1960
http://www.thebrainmatters.
Brain Injury Association of America
1608 Spring Hill Road
Vienna, VA 22182
Toll-Free: 1-800-444-6443
http://www.biausa.org/
Brain Trauma Foundation
708 Third Ave.
New York, NY 10017
Phone: 212-772-0608
http://www.braintrauma.org/
Getting a Second Opinion
A second opinion should be considered when deciding on a high-risk procedure like surgery or you want another opinion on your treatment options. It will also provide you with peace of mind. Multiple studies make a case for getting additional medical opinions.
In 2017, a Mayo Clinic study showed that 21% of patients who sought a second opinion left with a completely new diagnosis, and 66% were deemed partly correct, but refined or redefined by the second doctor.
You can ask your primary care doctor for another doctor to consider for a second opinion or ask your family and friends for suggestions. Another option is to use a Telemedicine Second Opinion service from a local health center or a Virtual Care Service.
References
- Abel, D. (April 28, 2010). Bill addressing student concussions advances. The Boston Globe. (accessed on June 29, 2010).
- Center for the Study of Traumatic Encephalopathy, Boston University, “20 More NFL Stars to Donate Brains to Research”, (accessed on June 29, 2010).
- McKee, A.C., Cantu, R.C., Nowinski, C.J., Hedley-Whyte, E.T., Gavett, B.E., Budson, A.E. Santini, V.E., Lee, H., Kubilus, C.A., & Stern;, R.A. (2009). Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury. Journal of Neuropathology and Experimental Neurology 68:7, 709-735.
- Los Angeles Times Staff and Wire Reports (June 28, 2010). Bengals’ Henry had chronic brain injury. Los Angeles Times.
- Sportslegacy.com, “Chronic Traumatic Encephalopathy”, (accessed on June 29, 2010).
- Telander, R. (June 25, 2010). What football did for us and … what football did to us: the story of the 1968-1970 Northwestern Wildcats. Sun Times. (accessed on June 29, 2010).
- Zeigler, T. (June 22, 2009). Chronic traumatic encephalopathy: possible consequences of recurrent concussion. Suite101.com.
