
Orbital blowout fracture
Last Updated on August 12, 2024 by The SportsMD Editors
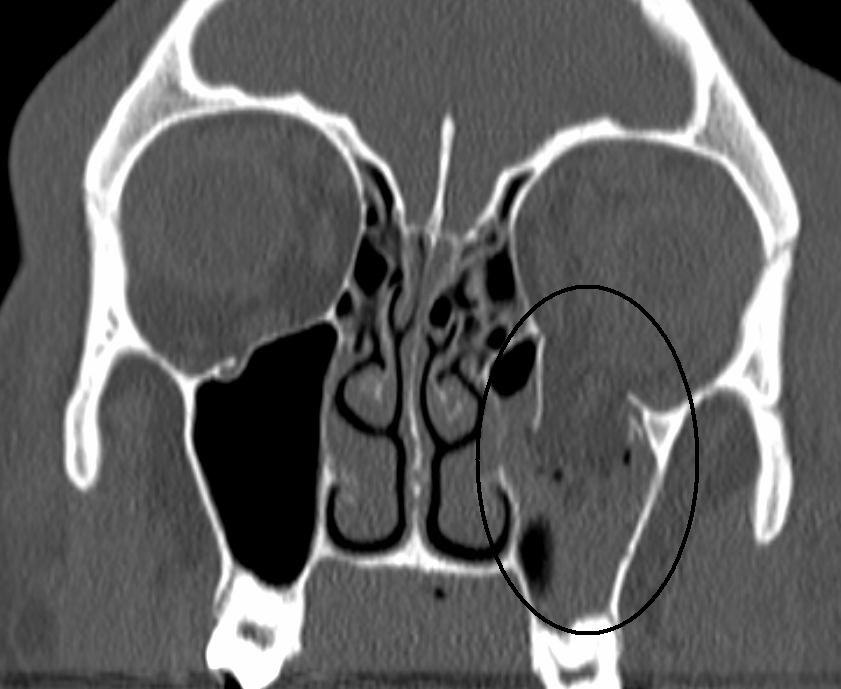
The orbit is the frontal part of the skull that provides structure and a boney pocket for the eyeball to sit in. Fractures can occur anywhere around the orbital walls but are most common to the orbital floor because it has the weakest bone structure.
Eye injuries resulting from orbital blowout fracture
Several serious injuries can occur to the eye as a result of the blunt force directly to the eyeball. The injuries include:
• Hyphema (hemorrhage into the anterior chamber)
• Retinal detachment
 A hyphema can result from the impact of a small ball directly into the eye. Within a few hours of impact, blood settles into the anterior chamber of the eyeball. This is a very serious eye injury requiring hospitalization, bed rest, bilateral patching of the eyes, and sedation. This condition usually resolves itself within a few days.
A hyphema can result from the impact of a small ball directly into the eye. Within a few hours of impact, blood settles into the anterior chamber of the eyeball. This is a very serious eye injury requiring hospitalization, bed rest, bilateral patching of the eyes, and sedation. This condition usually resolves itself within a few days.
A retinal detachment is another serious injury that can occur from blunt trauma to the eye, but may occur several months or years post-injury. The retina is the nerve bundle connecting the eyeball to the brain. Without it, the athlete would not be able to see.
A retinal detachment may include the athlete seeing “flashes of light” or the appearance of a “curtain” dropping. The athlete may also complain of “floaters” in his/her vision. Athletes with these symptoms should be immediately treated by covering both eyes with patches and referred to an ophthalmologist for surgical repair.
Symptoms of orbital blowout fracture
Any time an athlete receives a high force direct blow to the eye, a fracture should be suspected. The signs and symptoms of an orbital blowout fracture include:
• Immediate severe swelling
• Bleeding
• Recessed eyeball
• Inferiorly positioned eyeball
• Limited ocular movements (inability to lookup)
• Absent eye movements
• Double vision
• Numbness of the cheek
Who gets an orbital blowout fracture
The most common cause of an orbital blowout fracture is blunt force contact with an object larger than the orbit. Sports with these types of objects include tennis, racquetball, baseball, cricket, squash, and softball. The orbit can “blow-out” and fracture when one of these balls directly hits the eye at high speed effectively blowing the contents of the eye inward resulting in a fracture of the orbital floor.
An orbital blowout fracture can also occur to athletes in contact team sports when an athlete runs full force into a fist or elbow as in the sport of basketball. A direct blow to the face in fighting sports can also cause a “blow-out.”
Treatment for orbital blowout fracture
Because the amount of force required to fracture the orbit is significant, emergency medical services should be immediately called and care should be taken to also evaluate the athlete for a possible concussion, and/or brain injury.
To determine if the athlete has any signs and symptoms of concussion check for the following:
• Dizziness
• Headache
• Confusion
• Nausea
• Ringing in the ears
• Inability to answer simple questions
If any of the above symptoms are present, assume that the athlete might also have a concussion.
Gauze should be gently applied to the injured area to help stop any bleeding that may be present. Crushed ice can also be applied to reduce the amount of swelling but care must be taken not to increase the pressure to the eye.
If there is excessive bleeding, place a soft object under the athlete’s head and roll the athlete onto his/her side so that the blood can flow easily onto the ground and not back into the throat of the athlete.
Another aspect of immediate treatment for a seriously injured athlete is treating for shock. Athletes with serious injuries may go into shock because of the blood loss and/or the psychological impact of the injury.
Keeping the athlete calm by talking softly and slowly with an even pace is one effective way to comfort an athlete. The conversation should focus on anything but the injury. The goal of care during this time is to keep the athlete’s breathing pattern regular. A calm athlete should have respirations between 12 and 15 per minute.
Another way to ensure that the athlete stays calm is to remove all people from the scene who are not directly involved in caring for the athlete. Poorly timed comments or outbursts from teammates can alone send an athlete into psychological shock.
Surgery for orbital blowout fracture
Surgery will most likely be required to repair the fracture to the orbital floor and release any muscles and/or nerves that may have been compromised as a result of the fracture.
Returning to sports after orbital blowout fracture
The athlete’s safe return to sports will be dependent on the severity of the fracture and/or eye damage. The athlete should follow the specific instructions provided by his/her physician for the type and intensity of activity allowed until a full recovery has been made.
Getting a Second Opinion
A second opinion should be considered when deciding on a high-risk procedure like surgery or you want another opinion on your treatment options. It will also provide you with peace of mind. Multiple studies make a case for getting additional medical opinions.
In 2017, a Mayo Clinic study showed that 21% of patients who sought a second opinion left with a completely new diagnosis, and 66% were deemed partly correct, but refined or redefined by the second doctor.
You can ask your primary care doctor for another doctor to consider for a second opinion or ask your family and friends for suggestions. Another option is to use a Telemedicine Second Opinion service from a local health center or a Virtual Care Service.
Get a Virtual Sports Specialized appointment within 5 minutes for $29
 When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
References
- Anderson, M.K., Hall, S.J., & Martin, M. (2009). Foundations of Athletic Training: Prevention, Assessment, and Management. (3rd Ed). Lippincott Williams & Wilkins: Philadelphia, PA
- Bahr, R., & Maehlum S. (2004). Clinical Guide to Sports Injuries. Human Kinetics: Champaign, IL.
- Brukner, P., & Khan, K. (2004). Clinical Sports Medicine (revised 2nd Ed.). McGraw Hill: New York, NY.
