
Torn Achilles Tendon
Last Updated on August 12, 2024 by The SportsMD Editors
David Beckham is one of the many athletes who suffered from a torn Achilles tendon. The torn Achilles tendon requires surgical repair and rehabilitation that likely requires 6 – 9 months before return to competitive play.
While an Achilles tendon injury can be seen in almost all levels of competitive athletes, they have been historically linked with the “weekend warrior” athlete who may be somewhat de-conditioned. Recognition and treatment of an Achilles tendon injury is very important, as neglected or unrecognized ruptures can cause many future problems with both daily activities and sports competition.
What is the anatomy and function of the Achilles tendon?
The Achilles tendon connects the muscles of the calf and to the heel bone. The tendon is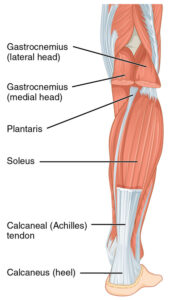 large and must be able to withstand and transmit the large forces generated by these powerful muscles to move the foot. These forces can be many times our own body weight. The tendon is particularly active with pushing down (plantar flexion) of the foot, and is therefore critical to perform in all sports, especially those in which jumping is critical. Correspondingly, sports such as basketball, track and field, and volleyball place high stresses on the Achilles tendon with jumping and landing, and are likely the highest risk for tendon injury. However, a torn achilles tendon has been reported with virtually every sport.
large and must be able to withstand and transmit the large forces generated by these powerful muscles to move the foot. These forces can be many times our own body weight. The tendon is particularly active with pushing down (plantar flexion) of the foot, and is therefore critical to perform in all sports, especially those in which jumping is critical. Correspondingly, sports such as basketball, track and field, and volleyball place high stresses on the Achilles tendon with jumping and landing, and are likely the highest risk for tendon injury. However, a torn achilles tendon has been reported with virtually every sport.
The Achilles tendon is located just beneath the skin and can be palpated just above the heel bone. It is nourished by a blood supply from an enveloping sheath of tissue (paratenon), although an area approximately 2 to 4 centimeters above the tendon’s insertion into the heel bone is the least well-perfused (“watershed” area). For this reason, this area of limited healing potential is a common location for tendon ruptures. The location of the tendon directly beneath the skin is also an important consideration for wound healing in the surgical treatment of ruptures.
What is an Achilles tendon injury?
An achilles tendon injury is a disruption in the integrity of the tendon somewhere between the muscle bellies and the heel bone (calcaneus). Most commonly, tears occur at the muscle-tendon junction 2 to 4 centimeters above the insertion into bone, but they can occur as avulsions directly from the calcaneus.
Tears can result from trauma or transection injuries that extend through the skin and underlying tendon. More commonly however, athletes suffer these injuries during sporting activities. Up to one-third of the athletes who suffer a rupture complained of some injury or symptoms in the tendon in the preceding weeks, suggesting that a preceding event may place the Achillies tendon at risk for rupture. Chronic inflammation or irritation of the tendon for repetitive activities (“Achilles tendinitis”) can also weaken the tendon and render it vulnerable to rupture as well.
What places me at higher risk for an Achilles Tendon Injury as an athlete?
Virtually anyone can suffer an achilles tendon injury, but certain pre-existing factors can place an athlete at greater risk and should be considered. These include:
• De-conditioning with weakness of the calf muscles, a common problem in “weekend” athletes who have not been training.
• Injections of steroids in or around the Achilles tendon – these can weaken the tendon and increase the risk of rupture with provocative activities, and should generally be avoided.
• Pre-existing Achilles tendinitis (inflammation of the tendon) with secondary degeneration and weakening of the tendon over time.
• Certain antibiotics (fluoroquinolones – Ciprofloxacin, Levofloxacin, Ofloxacin, etc) can place tendon at higher risk of injury
• Gout
• Hyper-parathyroidism
• Diabetes
How does an Achilles Tendon injury occur in athletes?
Most of the time, athletes will suffer an achilles tendon injury when a significant force is placed on the leg with the knee extended and foot pulled up (dorsi-flexed). This usually happens when awkwardly landing from a jump, and stresses the tendon when it is maximally stretched. This is a common occurrence and the basketball court.
Although Achilles tendon ruptures have been classically associated with the “weekend” athlete that is over the age of 30, they are certainly not restricted to them. Professional, well-conditioned athletes have suffered from them as well. These include NFL players Vinny Testaverde and Takeo Spikes, tennis champion Boris Becker, and many all-star NBA players, including Dominique Torn , Elton Brand, and Christian Laettner (Pictures).
What are the symptoms of an Achilles Tendon rupture in athletes?
The symptoms of an Achilles tendon rupture are generally not subtle. The athlete will usually complain about a “popping” that could be heard and felt when jumping or landing on the court or field. Up to one-third of the time, the athlete will have complained of some pain or symptoms in the Achilles in the prior weeks – it is thought that this inciting event may render it vulnerable to injury. The athlete will immediately complain of weakness with pushing off on the foot (plantar-flexion), reflected in difficulty walking and an inability to jump with the involved leg. Often there is a palpable defect at the location of rupture just above the heel bone, with loss of integrity of the “taut band” just deep to the skin. Examination of the opposite, normal side will help to detect these differences.
Some classic findings of an Achilles Tendon injury have been described. These include:
• Thompson Test – Normally, squeezing the calf muscle in the seated athlete will cause the foot to flex down (plantar-flex). In the setting of an Achilles rupture, however, no movement of the foot will occur.
• Hyper-Dorsiflexion Sign – With the athlete lying on their stomach, both knees are flexed up. The injured foot can be pushed down (dorsi-flexed) further than the normal side.
Are imaging studies useful?
Imaging studies can be useful as confirmatory tests for the diagnosis and to determine the location of the achilles tendon injury. Plain x-rays can help to rule out a “bony” avulsion fracture, but are of limited utility. Magnetic resonance imaging (MRI) and ultrasound are the most common imaging modalities used to visualize an Achilles tendon injury. Ultrasound (US) not only allows visualization of the tear, but is also dynamic and permits examination with active attempts at plantar-flexion and dorsi-flexion of the foot. MRI is more than 98% sensitive in diagnosing Achilles tendon rupture and can accurately be used to determine the location of rupture and severity of tendon retraction. This information can be helpful in planning for an Achilles tendon surgery repair.
Torn Achilles tendon treatment
Treatment options for an Achilles tendon injury are quite simple: operative or nonoperative. Some prompt treatment is important, however, as a torn Achilles tendon will seldom heal on its own. With rupture, the muscle belly and tendon retract proximally into the calf and leave a large “gap” defect that cannot heal. Furthermore, waiting for a long time before seeking medical attention (“chronic” rupture) or failing to recognize the injury can compromise treatment options – the tendon becomes stiff and scarred and sometimes cannot be repaired primarily (“end-to-end”).
Nonsurgical options offer the advantage of avoiding the complications of surgery. Typically, the foot is kept in a down position (plantar-flexed) to approximate the ruptured tendon ends as close as possible, and immobilized in a cast or rigid boot until healing occurs. The major limitation of nonoperative treatment, however, remains the risk of incomplete or no healing, and is a significant concern when there is significant tendon retraction. Correspondingly, the risk of recurrent rupture is higher with nonoperative treatment. This option is generally NOT pursued by athletes, given their desire to return to sporting and at-risk activities, and to therefore have the strongest repair possible.
Achilles tendon surgery offers the benefits of an immediate and secure “end-to-end” repair of the ruptured tendon. This allows for a predictable course of recovery and decreased risk of repeat rupture. The main risk of Achilles tendon surgery, however, relates to the surgical wound and healing. The Achilles tendon is directly beneath the skin, and the skin flaps for a repair can have a tenuous blood supply that can place healing of both the skin and tendon at risk. For this reason, meticulous handling of the skin and surrounding tendon sheath (“paratenon”) with a surgical repair is of critical importance.
What is nonoperative treatment and what outcome can I expect as an athlete?
Nonoperative treatment may be reasonable with an Achilles tendon injury that (i) have minimal retraction and gapping between the tendon ends, or (ii) older, low-demand patients with multiple medical comorbidities that are at greater risk for surgical complications. Athletes who expect to return to competitive, jumping sports typically will not elect this option due to the greater risk of recurrent rupture.
The foot is immobilized in the “down position” (equinus or plantar-flexed) to approximate the tendon edges as close as possible. The leg can be held in this position in a short arm cast or rigid boot. Weight-bearing on the leg is protected early, and gradually initiated after healing ensues typically at 4 to 6 weeks. The plantar-flexed position is gradually corrected to neutral over time. Rehabilitation to strengthen the muscles of the leg and calf is pursued after significant healing has occurred.
The results of nonoperative treatment are not perfect. Athletes cannot expect to fully return to competitive sports for one year or more. Furthermore, the risk of recurrent rupture can range from 4 to 30 percent. In addition, the tendon edges are often not completely approximately, resulting in a tendon that has healed in a “longer” position. This can reduce both the strength and endurance by as much as 30% compared to the normal, uninjured tendon.
Achilles tendon surgery
Achilles tendon surgery is typically the treatment of choice for athletes. Surgical repair usually allows for:
• A more predictable postoperative course of healing
• Secure “end-to-end” repair of the tendon
• Earlier return to sports
• Lower risk of recurrent tendon rupture
• Earlier and more predictable return of muscle power
Both percutaneous and open repair techniques to repair the tendon have been described. The motivation for percutaneous techniques has been to avoid the surgical wound and associated risks of wound infection or dehiscence at this location just above the heel bone. The blood supply of the skin in this location is tenuous, and can be at risk for sloughing if not carefully handled during open Achilles tendon surgery. While percutaneous techniques may protect the skin, they can place the adjacent nerves and vessels at greater risk of injury. The sural nerve is particularly at risk as it lies just lateral the Achilles tendon.
Open surgery is typically performed by making an incision just medial to the tendon. A medial incision avoids risk to the sural nerve and protects it from the risk of abrasion immediately on the backside of the Achilles tendon. The skin flaps are handled very gently to avoid trauma and injury to its blood supply. The enveloping sheath of the Achilles tendon (paratenon) is identified below and incised longitudinally over the tendon defect. The paratenon is also carefully handled and preserved so that it can be closed after tendon repair – this sheath nourishes the healing tendon and provides a protective layer between the tendon and overlying skin. A collection of blood (hematoma) from the trauma is typically encountered and irrigated away to visualize the ends of the ruptured tendon. The proximal end can sometimes “re-coil” deep into the calf and may need to retrieved into the wound. Any scar and adhesions of the ruptured tendon ends should be broken to allow full mobilization and “end-to-end” approximation of the tendon under minimal tension. Grasping sutures are then placed into both tendon ends and tied together to approximate the tendon to re-create its native, resting length. While various techniques and suture configuration have been described, the ultimate common goal is to resist gap formation and confer sufficient strength to the repair until interval healing of tendon occurs.
Repairs of chronic or neglected ruptures are more difficult. In certain cases, the tendon stumps can be so retracted, stiff, and scarred that they cannot be brought “end-to-end” for a primary repair. In these circumstances, augmentation with other tissue or tendon transfer from another muscle may be required and is usually associated with a less optimal result.
Get a Virtual Sports Specialized appointment within 5 minutes for $29
 When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments are within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments are within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
What is involved in postoperative rehabilitation?
A plaster splint is typically used to protect the wound for the first one to two postoperative weeks. After satisfactory wound healing is confirmed, the athlete is transitioned to a short leg cast or protective boot and protected weight-bearing with crutches is allowed for the next 6 to 8 weeks. No active plantar flexion and passive stretching of the Achilles tendon repair are encouraged during this time. Roll-A-bouts can be useful during this period to improve mobility and completely protect the healing tendon from weight-bearing. At approximately 6 weeks, gentle active plantar flexion and tendon stretching are initiated. Isotonic dorsiflexion and full weight-bearing in the protective boot are gradually allowed as well. By 3 months, muscle strengthening and proprioceptive training are initiated. These exercises can include:
• Isotonic plantar and dorsi-flexion exercises
• Isokinetics
• Balance Board and Perturbation Training (Read article)
• Stairmaster or Versiclimber
Achilles tendon surgery recovery
Return to sport is highly variable, and depends upon the type and severity of the achilles tendon injury, associated comorbidities, strength and rehabilitation, as well as treatment pursued. In general, healthy athletes who choose nonoperative treatment cannot expect a full return to sports for one year. On the other hand, an uncomplicated surgical repair in a healthy athlete often permits return to sport at 6 to 9 months.
Can I prevent an Achilles tendon injury?
Unfortunately, it is hard to anticipate and therefore “prevent” an Achilles tendon rupture. However, there has been some evidence to support that de-conditioning, loss of proprioception, and weakness of the calf musculature may increase the vulnerability to injury during exertion in sports. For this reason, staying well-conditioned and balanced with a steady training program is the most effective way to minimize the risk of an Achilles rupture. Nonetheless, even an athlete in “tip-top” condition can suffer an unfortunate, high-load achilles tendon injury!
It is also advisable to avoid fluoroquinolone antibiotics which can predispose to risk of tendon injury with provocative activities.
Below are some SportsMD calf stretching and strengthening videos
Alternate Positions for Calf Stretches: The Soleus & Calf Muscle
Strengthen Your Calf Muscle with Progressive Calf Raises
Questions and Answers
When discussing a torn Achilles tendon with a healthcare provider, asking questions is crucial to understand your condition and treatment options. Here are some questions you can ask, along with potential answers:
- What is a torn Achilles tendon?
- A torn Achilles tendon is a rupture or tear of the large tendon that connects the calf muscles to the heel bone (calcaneus).
- What caused my Achilles tendon tear?
- Achilles tendon tears often result from forceful or sudden movements, overuse, or pre-existing tendon weaknesses.
- How was the Achilles tendon tear diagnosed in my case?
- Diagnosis typically involves a physical examination and may include imaging studies like ultrasound or MRI.
- What symptoms should I expect with a torn Achilles tendon?
- Symptoms may include sudden, severe pain in the back of the calf or heel, swelling, and difficulty pointing the toes downward.
- Is surgery necessary for a torn Achilles tendon?
- The need for surgery depends on the extent of the tear, your age, activity level, and other factors. Some partial tears may be managed conservatively, while complete ruptures usually require surgery.
- What are the treatment options for a torn Achilles tendon?
- Treatment options may include surgery, casting or bracing, physical therapy, and activity modification.
- How long will the recovery process take, and what can I expect during this time?
- Recovery time varies based on the treatment approach and the extent of the tear. It can range from several months to a year or more. Physical therapy is often necessary.
- What restrictions or limitations should I expect during the recovery period?
- Your doctor will explain any restrictions on weight-bearing activities and exercise to protect the healing tendon.
- What are the potential complications associated with treatment and recovery?
- Complications can include infection (for surgery), re-rupture, or stiffness. Your doctor can provide more information.
- What is the long-term outlook for a torn Achilles tendon?
- With appropriate treatment and rehabilitation, many individuals can expect a good recovery with restored strength and function.
- Do I need a follow-up appointment, and when should it be scheduled?
- Establish a plan for post-treatment follow-up appointments to monitor your progress and make any necessary adjustments to your care.
Always consult with your healthcare provider for personalized answers to these questions, and feel free to ask additional questions or seek clarification on any points you don’t fully understand. Effective communication with your doctor is essential for your understanding and overall care.
References:
Inglis A, Scott W, Sculco T, Patterson A. Ruptures of the tendoachilles. An objective assessment of surgical and non-surgical treatment. J Bone Joint Surg Am 1976 Oct; 58(7): 990-3.
Nistor L. Conservative treatment of fresh subcutaneous rupture of the Achilles tendon. Acta Orthop Scand. 1976 Aug;47(4):459-62.
Nistor L. Surgical and non-surgical treatment of Achilles Tendon rupture. A prospective randomized study. J Bone Joint Surg Am. 1981 Mar;63(3):394-9.
