
Subdural Hematoma
Last Updated on August 12, 2024 by The SportsMD Editors
A subdural hematoma (collection of blood like clots) is a serious brain injury that can occur with any head traumatic accident including a serious head injury in athletics. Although exceedingly rare, other than a concussion, it is one of the most common major head injuries that can occur in athletics. Johan Frazen of the Detroit Red Wings in the 2008 NHL playoffs missed time due to a subdural hematoma. This fall, 10 year old David Sumner, a youth football participant, sustained an acute subdural hematoma during practice and later that day passed away. Some estimate that 1/5 of all major head injuries (concussions, epidural hematomas, subdural hematomas, etc.) in children occur during sports.
Who gets a subdural hematoma?
A subdural hematoma is caused by a traumatic blow to the head against an athlete during competition or practice. Therefore, athletes involved in collision sports are at most risk of a subdural hematoma. Therefore athletes participating in sports like boxing, mixed martial arts, football, and rugby are at the highest risk of sustaining a subdural hematoma. However, athletes in almost any sport can get a subdural hematoma if they sustain a traumatic blow to their heads. Examples could be a bicycle accident in cyclers, a ball or bat to the head in softball or baseball, a kick to the head in soccer or a car wreck in racing sports.
Symptoms of subdural hematoma
Symptoms from a subdural hematoma that cause a change in personality or intellect are most often seen as lethargy, difficulty with concentration and apathy. An injured athlete can also display confusion, become disorientated or show increased aggressiveness. They may have difficulty with short-term memory or simple calculations. The patient may also have an altered level of consciousness.
Relevant anatomy of the region
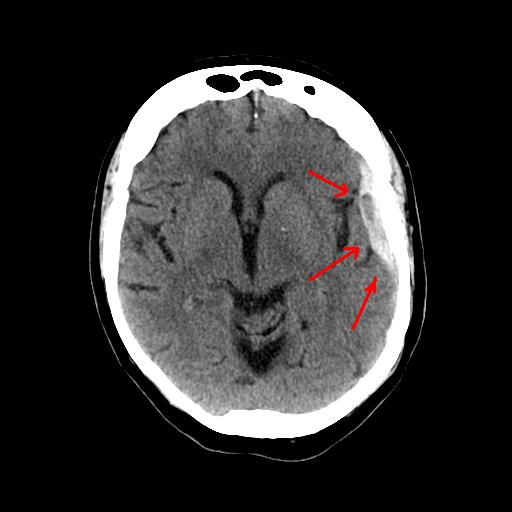 The brain resides within the cranium (composition of skull bones) and it sits within a protective layered sac with protective fluid (cerebrospinal fluid- CSF) known as the meninges. Although comprised of various structures (cortex, cerebellum, basal ganglia, corpus collosum, limbic system, brain stem) and lobes (parietal, frontal, temporal, occipital), the majority of the brain’s mass is composed of the cerebral cortex. The meninges are composed of 3 layers, the pia mater, arachnoid mater, and dura mater (dura for short) surrounding the brain from deep to superficial as listed. The dura mater, or “tough mother”, is the outermost and toughest layer that surrounds the brain and the spinal cord and contains the CSF. A subdural hematoma usually occurs when torn bridging veins within the subdural space leak blood between the dura and the arachnoid mater layers. In contrast, another often discussed intracranial bleeding injury due to head trauma is an epidural hematoma due to bleeding outside the dura mater layer between the dura and the skull. The image shows a CT Scan of the brain with subdural hematoma.
The brain resides within the cranium (composition of skull bones) and it sits within a protective layered sac with protective fluid (cerebrospinal fluid- CSF) known as the meninges. Although comprised of various structures (cortex, cerebellum, basal ganglia, corpus collosum, limbic system, brain stem) and lobes (parietal, frontal, temporal, occipital), the majority of the brain’s mass is composed of the cerebral cortex. The meninges are composed of 3 layers, the pia mater, arachnoid mater, and dura mater (dura for short) surrounding the brain from deep to superficial as listed. The dura mater, or “tough mother”, is the outermost and toughest layer that surrounds the brain and the spinal cord and contains the CSF. A subdural hematoma usually occurs when torn bridging veins within the subdural space leak blood between the dura and the arachnoid mater layers. In contrast, another often discussed intracranial bleeding injury due to head trauma is an epidural hematoma due to bleeding outside the dura mater layer between the dura and the skull. The image shows a CT Scan of the brain with subdural hematoma.
Causes of subdural hematoma
A subdural hematoma occurs when a traumatic blow to an athlete’s head causes the tearing of bridging blood vessels (usually veins) between the cerebral cortex and the covering of the brain, the dura, otherwise known as the subdural space. When these blood vessels tear, they bleed into the subdural space and create a mass or clot that compresses the cerebral cortex. In older patients who have undergone shrinkage of their cerebral cortex as is normal over time, their symptoms are often due mainly to the compression of the brain by the clot. Often younger patients who have normal sized cerebral cortices therefore have less room for the clot to swell and their symptoms are often due to an actual injury to the brain itself as opposed to from the bleeding subdural injury.
Treatment for subdural hematoma
Any athlete with a suspected subdural hematoma should be taken immediately to a nearby emergency room for an immediate work-up of their injury. It is important to know if the athlete has a known coagulopathy: blood clotting disorder such as from certain medications like aspirin, Coumadin, heparin or from an underlying medical condition. This is an important risk for developing a subdural hematoma. Blood work and other laboratory tests are important to obtain immediately in the ED. Once the athlete is confirmed to be medically stabilized, then a CT scan without contrast (enhancing dye) is obtained to look for evidence of blood within the skull, fractures and also signs that there may be compression of the brain from a hematoma or mass.
An MRI scan is much less frequently used to diagnose a subdural hematoma. In the acute setting an MRI scan takes much longer to obtain for various reasons. Also, it is important to know of any metallic implants or pieces in the patient’s body which can affect the MRI. This may not be possible in the acute setting with a confused patient. MRI is however superior to CT scan to evaluate injury to the brain tissue itself. Also, it can be useful for identifying any mass that may not be due to a hematoma such as an infection or tumor.
Longer term management of a subdural hematoma
A large subdural hematoma that causes compression of the brain (mass effect) and significant symptoms for the athlete often requires surgery by a neurosurgeon to evacuate the hematoma. If a patient has a bleeding disorder (coagulopathy), either from a medication or a medical condition, then a transfusion with platelets and or fresh frozen plasma (clotting factors) may be necessary. Surgery depends on the location and other specifics regarding the hematoma and usually consists of either creating a window in the skull over the clot (craniotomy) or drilling/burring holes over the clot in the skull. The clot is then removed, and the patient’s intracranial pressure is then monitored closely for days afterward. After treatment for a subdural hematoma, the patient is also monitored for such complications as seizures, clot re-accumulation, and infection. Sometimes a second hematoma drainage procedure is necessary if the hematoma re-accumulates.
A smaller subdural hematoma that does not cause a mass effect on the underlying brain and those that have minimal symptoms may be monitored closely instead of treating them with immediate surgical evacuation. The patient then requires follow-up CT scans to be sure the hematoma is not enlarging and that it eventually resolves.
Prognosis and returning to sports
Subdural hematomas are especially serious injuries not only in athletes. Taking all patients, not only athletes, with a subdural hematoma the outcomes are often very guarded. The prognosis following treatment is best correlated with how the patient was on presentation. The Glascow coma scale (GSC) is a standardized assessment of a patient’s neurologic status that is used with many different head injuries and is the best predictor of how a patient will recover following a subdural hematoma. Other factors like elevated intracranial pressure, increased patient age, and abnormalities of the pupils are indicators of a poorer prognosis. The mortality rate following an acute subdural hematoma can be as high as 80% and survivors do not always regain the same level of pre-injury function.
Determining when an injured athlete can return to sports participation is a complex issue that requires the multidisciplinary input of the sports medicine physician, neurologist and or neurosurgeon, athletic trainer, coaches and family. The severity of the subdural hematoma plays a major role in this decision-making process. If an athlete is to return to athletics, he or she must be completely asymptomatic both at rest and with exertion as well as clear documentation on CT scan that the hematoma has resolved. The athlete must be brought along slowly and closely monitored to be sure that symptoms don’t redevelop after they return to athletics.
Recent news about Subdural Hematoma
The New York State Athletic Commission would be right back where it was with Magomed Abdusalamov. Let’s repeat that point so no one misses it. Suppose Sebastian Heiland suffered a subdural hematoma after being pounded in the head again and again … The New York State Athletic Commission is Still Courting Disaster – The Sweet Science
Getting a Second Opinion
A second opinion should be considered when deciding on a high-risk procedure like surgery or you want another opinion on your treatment options. It will also provide you with peace of mind. Multiple studies make a case for getting additional medical opinions.
In 2017, a Mayo Clinic study showed that 21% of patients who sought a second opinion left with a completely new diagnosis, and 66% were deemed partly correct, but refined or redefined by the second doctor.
You can ask your primary care doctor for another doctor to consider for a second opinion or ask your family and friends for suggestions. Another option is to use a Telemedicine Second Opinion service from a local health center or a Virtual Care Service.
Get a Virtual Sports Specialized appointment within 5 minutes for $29
 When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
When you have questions like: I have an injury and how should I manage it? How severe is it and should I get medical care from an urgent care center or hospital? Who can I talk to right now? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365, and appointments within 5 minutes. Learn more via SportsMD’s Virtual Urgent Care Service.
References
- Iantosca MR, Simon RH. Chronic subdural hematoma in adult and elderly patients. Neurosurg Clin N Am. 2000 Jul;11(3):447-54.
- Chen JC, Levy ML. Causes, epidemiology, and risk factors of chronic subdural hematoma. Neurosurg Clin N Am. 2000 Jul;11(3):399-406.
- Pierre Durand, Jr and Gregory J. Adamson. On-the-Field Management of Athletic Head Injuries. J. Am. Acad. Ortho. Surg., May/June 2004; 12: 191 – 195.
