
ACL Surgery
Last Updated on October 6, 2023 by The SportsMD Editors
The anterior cruciate ligament (ACL) is one of the four major ligaments that connect the bones of the knee joint. The ACL ligament helps to hold the bones in proper alignment and helps control the way your knee moves. The ACL provides stability to the knee and prevents excessive forward movement of the lower leg bone (tibia) in relation to the thigh bone (femur).
Causes of torn ACL
A torn ACL can be grouped into two categories: contact and non-contact. An example of non-contact injuries would be when an athlete rapidly decelerates, followed by a sharp or sudden change in direction (cutting). Noncontact torn ACL injuries have also been linked to heavy or stiff-legged landing as well as twisting or turning the knee while landing, especially when the knee is in the valgus (knock-knee) position. Contact injuries most commonly occur after a blow to the outside of the leg causing the knee to “buckle” and assume a valgus position.
Classifications of torn ACL
Most clinicians describe a torn ACL as either partial or complete. This is based on physical examination and imaging findings (discussed later).
Do women really tear their ACLs more than men?
Women in sports such as soccer, basketball, tennis and volleyball are significantly more prone to a torn ACL than men. The discrepancy has been attributed to differences between the sexes in anatomy, general muscular strength, reaction time of muscle contraction and coordination, and training techniques. Hormonal causes have also been investigated although it is still unclear what role they may play in an ACL tear if any. Lastly, women have a relatively wider pelvis, requiring the femur to angle toward the knees (knock knee) which may also be a predisposing factor towards a torn ACL.
How do I know if I have a torn ACL?
Patients who suffer an ACL injury often report hearing an audible pop followed by significant swelling. Afterwards, patients may complain of instability of the knee (i.e., a “wobbly” feeling) especially when trying to change directions during sporting activity. Continued athletic activity on a knee with a torn ACL can have devastating consequences, resulting in massive cartilage damage, leading to an increased risk of developing osteoarthritis later in life.
How will my doctor determine if I have a torn ACL?
Several diagnostic maneuvers help clinicians diagnose a torn ACL. In the anterior drawer test, the examiner applies an anterior force on the proximal tibia with the knee in 90 degrees of flexion(picture). The Lachman test is similar, but performed with the knee in only about twenty degrees of flexion, while the pivot-shift test adds a valgus (outside-in) force to the knee while it is moved from flexion to extension. The Lachman and anterior drawer assess purely for translation, whereas the pivot shift test assesses for rotational instability. Any abnormal motion in these maneuvers suggests a tear.
The diagnosis is confirmed by MRI (magnetic resonance imaging) which also is used to assess for other ligament, meniscus, and cartilage pathology.
Treatment
Treatment without ACL surgery
Nonsurgical options may be used if the knee cartilage is undamaged, the knee proves to be stable during typical daily activities, and if the patient has no desire to ever again participate in high-risk activities (sports involving cutting, pivoting, or jumping). Nonsurgical treatment is typically only considered in cases of low grade partial injuries. If the nonsurgical option is recommended, the physician will recommend physical therapy, wearing a knee brace, and avoiding any provocative maneuvers.
The goal of physical therapy is to strengthen the muscles around the knee to compensate for the absence of an ACL. Initially the goal of physical therapy is to restore range of motion; after a period of time, the physician will prescribe a strengthening program that focuses on the hamstrings first and later the quadriceps, hip, and core musculature.
Most ACL-deficient athletes conclude that their knee continues to feel unstable, again confirming the important role of the ACL in normal knee stability. Therefore, most orthopaedic surgeons recommend ACL surgery treatment in the athletic population because repetitive insults to the knee as a result of ACL deficiency often result in meniscal and cartilage injury. Such injuries can ultimately lead to persistent pain, disability, and premature osteoarthritis. However, initially, sports injury treatment using the P.R.I.C.E. principle – Protection, Rest, Icing, Compression, Elevation can be applied to a torn ACL.
What’s involved with ACL surgery?
There are two main options for ACL graft selection: autograft and allograft. Autografts are 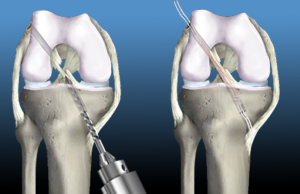 the patients’ own tissues, and the most common options include the middle third of the patella tendon and the hamstring tendons. Allografts are cadaveric tissue sourced from a tissue bank; the most common allograft tissue used for ACL reconstruction is Achilles tendon. Each method has its own advantages and disadvantages; patellar tendon autografts are the most common and often considered the gold standard for young highly competitive athletes. However, the site of the harvest is often painful for weeks after surgery and some patients can develop tendinitis or generalized knee pain that can be difficult to recover from. Such complications are generally avoided when using hamstring autografts, although some clinicians feel hamstring reconstructions become loose over time. It should be noted that many clinicians used both with an extremely high success rate and their use is often surgeon preference or bias.
the patients’ own tissues, and the most common options include the middle third of the patella tendon and the hamstring tendons. Allografts are cadaveric tissue sourced from a tissue bank; the most common allograft tissue used for ACL reconstruction is Achilles tendon. Each method has its own advantages and disadvantages; patellar tendon autografts are the most common and often considered the gold standard for young highly competitive athletes. However, the site of the harvest is often painful for weeks after surgery and some patients can develop tendinitis or generalized knee pain that can be difficult to recover from. Such complications are generally avoided when using hamstring autografts, although some clinicians feel hamstring reconstructions become loose over time. It should be noted that many clinicians used both with an extremely high success rate and their use is often surgeon preference or bias.
ACL surgery reconstruction using allograft tissue does carry a slightly higher infection risk but patients often recover the fastest of all the graft choices. Although not recommended for young, extremely active athletes, allograft reconstruction is often a popular choice for the older more sedentary athlete. Many patients worry about the transmission of disease from the allograft itself; although this has been reported in the literature, most clinicians feel such risk is extremely low and feel very comfortable using allograft tissue.
The ACL surgery is performed arthroscopically, with tunnels drilled into the femur and tibia at the original of the ACL footprints. The graft is then placed into position and held in place. There are a variety of fixation devices available, particularly for hamstring tendon fixation. These include screws, buttons and post fixation devices. The graft typically attaches to the bone within six to eight weeks. The original collagen tissue in the graft acts as a scaffold and new collagen tissue is laid down in the graft with time.
What is double bundle ACL reconstruction and do I need it?
Since the native ACL consists of two bundles, some clinicians have advocated a double bundle reconstruction which places two separate grafts during surgery instead of just one. Although biomechanical studies have shown an advantage in this technique, no clinical studies have demonstrated it to be superior to standard single graft techniques. Furthermore, it is unclear what the potential disadvantages of a double bundle technique are. Most clinicians still use a single graft approach with very high success. It is important to consult your surgeon to discuss what his/her preference is and why.
What will physical therapy be like after ACL surgery?
After ACL surgery, the knee joint loses flexibility, and the muscles around the knee and in the thigh tend to atrophy. All treatment options require extensive physical therapy to regain muscle strength around the knee and restore range of motion (ROM). For some patients, the lengthy rehabilitation period may be more difficult to deal with than the actual ACL surgery.
External bracing is recommended for athletes in contact and collision sports for a period of time after reconstruction. It is important however to realize that many of the specific rehabilitation protocols are physician dependent. Generally speaking, most surgeons will prescribe a brace and crutches for post ACL surgery recovery for approximately one month. After that, a rehabilitation period of six months to a year is required to regain pre-surgery strength and use.
Rehab after ACL surgery can vary widely, but there are some general principles that are true for most patients having surgery for treatment of an ACL. Start strengthening exercises only after you have your health professional’s approval. The list below provides links to specific rehab ACL video exercises:
When can I return to athletics?
Most clinicians allow for a competitive return to sport at 6 to 7 months. Also, be sure to take a look at the SportsMD Video on proper icing of an ACL injury.
Can a torn ACL be prevented?
Athletes can lower their risk of torn ACL by participating in performance drills that focus on improving lower extremity strength, agility, flexibility, and power. The Santa Monica ACL Prevention Project developed an ACL Injury Prevention Program specifically designed for female soccer players that can be applicable for all athletes both male and female.
Getting a Second Opinion
A second opinion for ACL surgery should be considered when deciding on a high-risk procedure like surgery or you want another opinion on your treatment options. It will also provide you with peace of mind. Multiple studies make a case for getting additional medical opinions.
In 2017, a Mayo Clinic study showed that 21% of patients who sought a second opinion left with a completely new diagnosis, and 66% were deemed partly correct, but refined or redefined by the second doctor.
You can ask your primary care doctor for another doctor to consider for a second opinion or ask your family and friends for suggestions. Another option is to use a Telemedicine Second Opinion service from a local health center or a Virtual Care Service.
Get a Telehealth Appointment or Second Opinion With a World-Renowned Orthopedic Doctor
 Telehealth appointments or Second Opinions with a top orthopedic doctor is a way to learn about what’s causing your pain and getting a treatment plan. SportsMD’s Telehealth and Second Opinion Service gives you the same level of orthopedic care provided to top professional athletes! All from the comfort of your home.. Learn more via SportsMD’s Telemedicine and Second Opinion Service.
Telehealth appointments or Second Opinions with a top orthopedic doctor is a way to learn about what’s causing your pain and getting a treatment plan. SportsMD’s Telehealth and Second Opinion Service gives you the same level of orthopedic care provided to top professional athletes! All from the comfort of your home.. Learn more via SportsMD’s Telemedicine and Second Opinion Service.
References
- A randomized controlled trial to prevent noncontact anterior cruciate ligament injury in female collegiate soccer players. Gilchrist J, Mandelbaum BR, Melancon H, Ryan GW, Silvers HJ, Griffin LY, Watanabe DS, Dick RW, Dvorak J. Am J Sports Med. 2008 Aug;36(8):1476-83.
- Robin V. West and Christopher D. Harner Graft Selection in Anterior Cruciate Ligament Reconstruction J. Am. Acad. Ortho. Surg., May/June 2005; 13: 197 – 207.
- Treatment of anterior cruciate ligament injuries, part I. Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nichols CE. Am J Sports Med. 2005 Oct;33(10):1579-602 Treatment of anterior cruciate ligament injuries, part 2. Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nichols CE. Am J Sports Med. 2005 Nov;33(11):1751-67
