
What is a rib stress fracture?
By Asheesh Bedi, MD and Benjamin Bissell, MD
Last Updated on August 12, 2024 by The SportsMD Editors
A rib stress fracture is rare, but can be seen in high-level athletes with significant demands of repetitive upper extremity activities, such as rowers, track and field, baseball, backpacking, dance, running, and windsurfing athletes. Stress fractures in the legs and feet of runners are much more common due to the constant, repetitive impact forces with each stride. A stress fracture is an area in the bone where it has become weakened and microscopic cracks have gradually formed because the bone is repeatedly loaded and stressed. This is different from a regular “traumatic” bone fracture or break in which one event causes the bone to crack all at once. The cracks in stress fractures are often so small that they can’t be seen on regular x-rays, but the area where the bone has built up some new bone (“callus”) as it tries to heal is sometimes visible. A stress fracture can progress to become a complete fracture if it is not allowed to heal with a period of rest. Stress fractures can occur in almost any bone.
Anatomy involved in rib stress fracture
Most commonly the first rib is the one involved in a rib stress fracture. There are 12 ribs 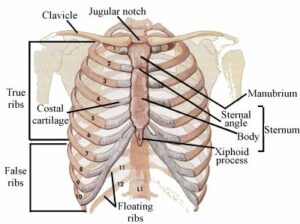 on the right and 12 ribs on the left. The first rib is the top one and it can barely be felt deep in the space behind and above the collar bone (clavicle). The first rib connects the spine in the back to the breast bone (sternum) in the front. Large blood vessels (subclavian artery and vein) travel right over the first rib as they go to the arm. These vessels have corresponding grooves in the first rib where the vessels travel over the rib. These grooves make the rib thinner and weaker in those regions. Normally, the bone can withstand these forces, but when a stress fracture has formed, the repeated stress on the bone exceeds the rate at which the bone can repair itself.
on the right and 12 ribs on the left. The first rib is the top one and it can barely be felt deep in the space behind and above the collar bone (clavicle). The first rib connects the spine in the back to the breast bone (sternum) in the front. Large blood vessels (subclavian artery and vein) travel right over the first rib as they go to the arm. These vessels have corresponding grooves in the first rib where the vessels travel over the rib. These grooves make the rib thinner and weaker in those regions. Normally, the bone can withstand these forces, but when a stress fracture has formed, the repeated stress on the bone exceeds the rate at which the bone can repair itself.
Rib stress fracture symptoms
Rib stress fracture symptoms include gradual onset of pain in the side of the neck and upper back and/or pain in the back of the shoulder. This may gradually increase or come and go for weeks to months. The pain gets worse with activity and gets better with rest. The pain may be worsened by deep breaths, using the arm overhead, or by coughing. Rarely, the athlete may feel a pop or snap if the stress fracture all of the sudden becomes a complete fracture.
When the physician examines the athlete, a complete exam of the shoulder, neck, and arm will rule out other causes of the pain. The athlete will have tenderness directly over the first rib (behind the collarbone at the base of the neck). Squeezing the trapezius muscle at the base of the neck may be painful.
What imaging is used?
If a stress fracture is suspected, x-rays of the rib will be taken. If the diagnosis is not clear, x-rays might also be taken of the neck and/or shoulder. On x-rays, a stress fracture may show up as a small crack, or the bone might be thickened in that area from trying to heal. If the stress fracture has gone on to become a complete fracture, there may be a very obvious crack visible. Oftentimes, however, the stress fracture doesn’t show up in the x-ray. In this case, a bone scan, MRI, or CT may be ordered.
A bone scan is a special test with a tracer that is injected into an IV. The tracer is taken up more strongly by areas of the bone that are trying to heal, so the stress fracture shows up as a bright spot. A CT scan is a special scan that shows the details of bone very well and can show small cracks and changes in bones. It can also show if there is an underlying cause of the fracture such as a bone cyst, but this is very rare. An MRI may also reveal areas of increased inflammation and swelling in response to the stress reaction in the bone.
What may predispose me to getting a rib stress fracture as an athlete?
A rib stress fracture is not common, but they have been reported in many sports that have repetitive vigorous shoulder motions. These sports include baseball (especially pitching), dancing, tennis, golf, rowing, backpacking, windsurfing, and other sports. They have also been seen in people that do a lot of shoveling.
Often, there is no clear cause for the stress fracture, but there are some factors that sometimes contribute. A sudden increase in weightlifting or training could predispose to stress fractures. Poor mechanics when participating in the sport may also increase the risk of stress fracture. A poor diet, eating disorders such as anorexia, lack of vitamin D, lack of calcium, and insufficient rest may contribute. In some female athletes who train extensively, amenorrhea (infrequent menstrual periods) may lead to weaker bones and a predisposition to getting stress fractures. Rarely, a disease or a biochemical imbalance may contribute to weaker bones.
Prevention
Many stress fractures could be avoided by watching for and correcting the factors discussed above. Work with a coach to be sure you are using the proper form and mechanics in your sport. Gradually increase training and weightlifting to give your body a chance to adjust. Get plenty of rest and be sure to eat a balanced nutritious diet with plenty of calcium and vitamin D. If a stress fracture is developing, it is important to recognize it and rest early to avoid further injury and the risk for secondary traumatic fracture.
Rib Stress Fracture Treatment
Rib stress fracture reatment without surgery is always the most appropriate first-line of treatment for a typical rib stress fracture. The key is “relative rest” which means don’t do anything that causes significant pain or discomfort. The goal is to let the rib rest so it can heal itself. If stress is continually placed on it, it never gets a chance to heal. This usually means a period of 4-6 weeks without throwing or weightlifting with the affected shoulder, but lower body workouts can usually be continued without interruption or they can be modified so they do not cause rib pain. Once there is no pain during regular activities, then light lifting and throwing, or other sport specific activities, can be gradually added. If pain recurs, then the athlete must back off again and give it more time. [amazon_link asins=’B00W963NZW,B0027CU1B2′ template=’ProductCarousel’ store=’sportsmd-20′ marketplace=’US’ link_id=’2f5331f8-d1fa-11e7-bddf-bb76617f6b4c’]
Other important elements of treatment include analyzing the training program, rest, and body mechanics of the athlete to identify and correct any contributing factors. Also, the diet should be examined to make sure nutrition is appropriate.
If the athlete has a history of multiple stress fractures or if the fracture is not healing, it may be appropriate to do some blood tests or special imaging to make sure there are not other, systemic factors involved.
The time for healing may vary significantly between athletes and must be individualized and discussed with the athlete’s physician. If the stress fracture is not visible on x-rays, the athlete might return to full sports participation in 8-12 weeks. If the stress fracture has become a complete fracture, it may take 6-12 months.
Is surgery needed for rib stress fractures?
In the vast majority of cases, surgery is not needed. Even if the bone doesn’t heal, the athlete can usually get back to their sport without surgery and without pain. However, there are some unusual reported cases of the bone healing with such a large mass of bone (“callus”) that it impinges the underlying nerves and vessels and requires a “decompressive” surgery.
Can Telemedicine Help?
Telemedicine is gaining popularity because it can help bring you and the doctor together quicker and more efficiently. It is particularly well suited for sports injuries and facilitating the diagnoses and treatment of those injuries. Learn more about speaking with a sports specialized provider via SportsMD’s 24/7 Telemedicine Service.
Read about a 1st Rib stress fracture today and decided to read more:
– baseball, tennis, kick boxing, also listed was ballet.
– Trap squeeze test listed as diagnostic test
-Most commonly occur in the depression for subclavian artery
– Can sometimes be seen on plain film#meded pic.twitter.com/BEc2nfTyzw— Caitlyn Mooney (She/Her) (@CaitlynMooneyMD) December 5, 2019
References:
- Coris EE, Higgins HW. First rib stress fractures in throwing athletes. Am J Sports Med. 2005;33:1400-1403.
- Prisk VR, Hamilton WG. Stress fracture of the first rib in weight-trained dancers. Am J Sports Med. 2008;36:2444-2447.
